Article type
Year
Abstract
Background:
For continuous outcomes with an established minimally important difference (MID), we have previously described the merits of reporting in MID units the pooled estimate of effect from trials employing more than one instrument with an anchor-based MID. However, many instruments do not have an established anchor-based MID, and our method thus far omits these studies. We describe here an approach that addresses this limitation.Methods:
Our approach relies on evaluation of the relationship between the anchor-based MID and the SD of the trials within a given meta-analysis. Based on this relationship, we infer the MID for trials having employed instruments without an anchor-based MID. We evaluated the consistency of magnitude of effects from studies using distribution and anchor-based instruments using a test for interaction. We applied this approach to two Cochrane meta-analyses.Results:
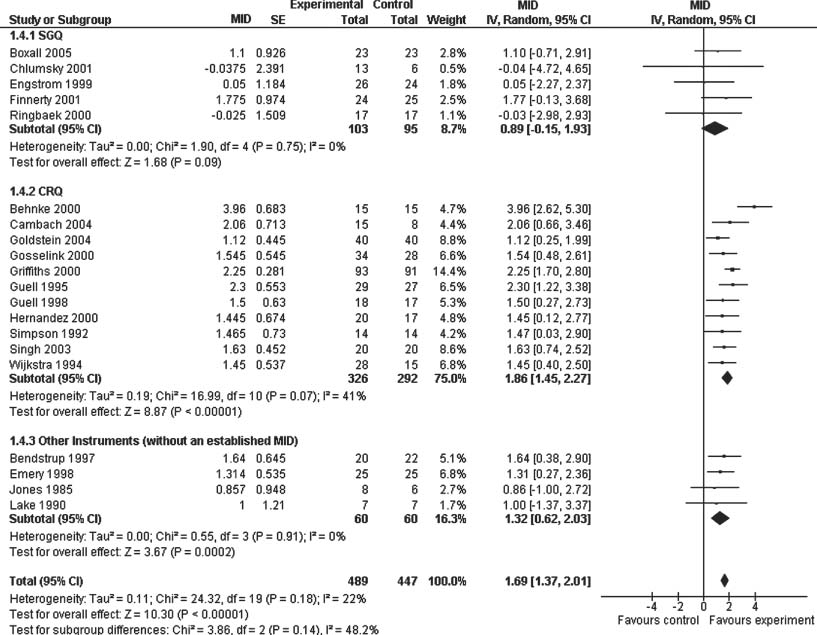
Of 20 trials involving respiratory rehabilitation, 16 employed instruments with an established anchor-based MID, and 4 trials did not. The pooled estimate was 0.89 (95% CI 0.15, 1.93) (St. Georgeás Questionnaire), 1.86 (95% CI 1.45, 2.27) (Chronic Respiratory Questionnaire) and 1.32 (95% CI 0.62, 2.03) (instruments without an established MID) (Figure1) (test for interaction p = 0.14$). The second example included 53 trials that examined the efficacy of Amitriptyline vs. other antidepressants; 16 used the 17-item Hamilton Rating Scale, 3 used Montgomery-Asberg Scale, and 34 used instruments without an established MID. The pooled estimate for each subgroup was 0.20 (95% CI 0.07, 0.32), -0.18 (95% CI -0.92, 0.57), and 0.17 (95% CI -0.02, 0.36) (Figure 2) (test for interaction p = 0.63).Conclusions:
The effect of the interventions was not significantly different between distribution and anchor-based instruments. For instruments without an anchor-based MID, the test for interaction suggests that we have appropriately imputed the MID, thus allowing for increased precision around the pooled estimate of effect.Images
{kind=link}