Article type
Year
Abstract
Background:
QUADAS was developed in 2003 to assess the quality of diagnostic test accuracy (DTA) studies included in systematic reviews. It includes 14 items covering risk of bias, variability and reporting. Personal experience, anecdotal reports, and feedback via the Cochrane Collaboration suggested that some elements required improvement.Objectives:
To update the QUADAS tool to produce QUADAS-2.Methods:
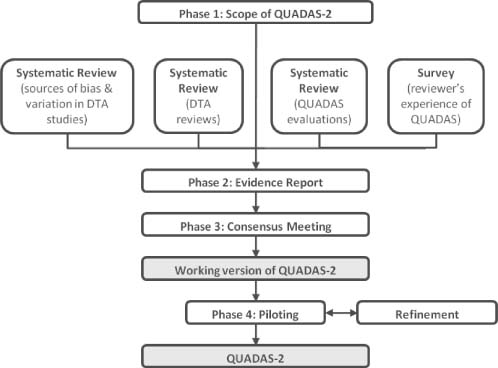
We used a four-phase approach to develop QUADAS-2 (Figure 1): defining the scope, developing the evidence base, face-to-face consensus meeting, and refinement through piloting. We established a broad team including methodological experts and review authors working on DTA reviews.Results:
We defined quality in terms of risk of bias and concerns regarding applicability. Based on the evidence we identified items for removal, items to be re-worked, and items to be considered for inclusion. Discussions at the face-to-face meeting informed decisions regarding the structure and content of QUADAS-2. After four rounds of piloting, agreement was reached on the final tool.QUADAS-2 consists of four domains covering: patient selection; index test; reference standard; and flow of participants through the study and timing of tests. All domains are assessed in terms of the risk of bias. Patient selection, index test, and reference standard are also assessed in terms of concerns regarding applicability to the review question. QUADAS-2 is applied in four phases: (1) summarise the review question; (2) tailor the tool to the review including production of review specific guidance; (3) construct a flow diagram for the primary study; and (4) assess risk of bias and concerns regarding applicability.Conclusions:
The development of QUADAS-2 was evidence based and included detailed piloting and refinement. We feel that QUADAS-2 is a considerable improvement on the original QUADAS tool and will allow more objective rating of the risk of bias and applicability of primary DTA studies.Images
{kind=link}