Article type
Year
Abstract
Background:
When introducing a new more sensitive test into practice, one concern is whether treatment harms outweigh benefits in the additional cases detected; particularly when the new test identifies a milder spectrum of disease, e.g. computed tomographic pulmonary angiography compared with ventilation/perfusion scanning for pulmonary embolism.Objective:
To demonstrate how the principles used to assess the applicability of treatment evidence to broader populations (1) can be used to assess claims of improved treatment using a new more sensitive test.Methods:
We defined the additional cases detected for treatment by the new test as the ‘new test-defined population’. Using published examples, we demonstrate how the principles used to appraise the applicability of treatment evidence to populations not included in treatment trials can help assess claims about treatment benefits using new tests.Results:
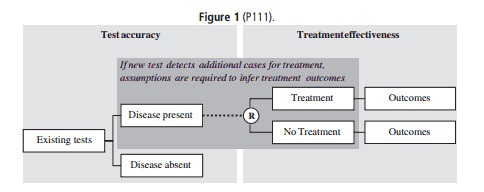
The treatment comparison for new test-defined populations is treatment change that will occur for patients based on the new versus existing tests (Fig. 1). When this evidence is only available for populations defined by the existing tests, two critical assumptions are:—The relative treatment effects are similar in the new test-defined population. Supportive information includes: (i) trials demonstrating the relative effectiveness of treatment in patients with similar disease characteristics; (ii) trials demonstrating the relative effectiveness of treatment is similar across different disease subgroups; and/or (iii) strong biological plausibility.—The baseline risk of disease events outweighs the harms of treatment. Relevant evidence includes: (i) disease characteristics/spectrum for the new-test defined population differ from the existing-test defined population; (ii) patient prognosis varies across the disease spectrum; (iii) treatment harms vary across the disease spectrum.Conclusions:
Reviewers can use these principles to make explicit statements about the evidence available and assumptions required to infer a more sensitive test will lead to improved outcomes, and decide whether further treatment trials are needed in the new test-defined population.Reference
1. Glasziou PP, Irwig L. An evidence-based approach to individualising treatment. BMJ 1995, 311: 1356–1359.
Images
{kind=link}